BOB Community CDI Analysis 2024/25
BOB Community Clostridioides difficile infection (CDI) Analysis, 2024/25
As per the UKHSA Annual epidemiological commentary1, nationally, Clostridioides difficile infection (CDI) cases have increased from 2020 to 2024 by 33%; this marks the highest overall case rate since 2011 both healthcare associated and community associated CDI cases. CDI cases are considered hospital-onset if they occur 4 or more days after admission to an acute trust (HOHA), or admitted to the reporting organization within the past 12 weeks (COHA), all others are categorised as community associated (COCA or COIA) as per UKHSA categorisation.
Overall, community cases have seen a 21% increase from 2021-2024 and have always shown a peak in the second quarter of the financial year (Jul-Sep). Community-onset cases now constitute the greater burden of all CDI for 2023/24, 59.9%. We are seeing a higher proportion of female cases than males across all age groups except in the aged 85 years, and a significant increase in females aged 15 to 44 years.
UKHSA data from the past 4 years show no significant changes in C. difficile ribotypes. Current hypothesis for the increase, suggest challenges in infection prevention during the pandemic, changes in antibiotic use, and improved CDI detection may be contributing factors.
Historically1, CDI was primarily an issue within the hospital setting with around 60.2% of infections defined as hospital-onset. Many of the interventions aimed at the reduction of CDI rates were targeted at the hospital setting, and as a result the sharp decline that has been observed has disproportionately affected hospital-onset infections compared to community-onset infections. Consequently, community-onset cases now constitute the greater burden of all CDI for the reporting period (59.9%).
Community Onset cases-CDI investigation process
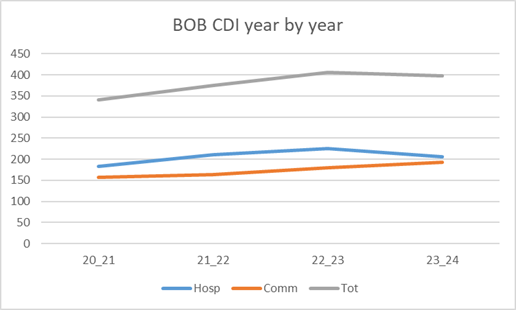
In Buckinghamshire Oxfordshire and Berkshire West Integrated Care System (BOB ICS), CDI increased year on year until 2023/24 when a total reduction from 405 to 398 was seen, although, community onset cases, continue to increase from 179 to 193, as seen in figure 1. The BOB Integrated Care Board (ICB) Infection Prevention & Control (IP&C) team investigate all community onset CDI cases, whilst the acute trusts review the healthcare categorised cases.
Previously, as the IP&C team do not have access to patient records, an email was sent to GP’s with a request to complete a ‘Post infection review’ form and the prior prescribing was reviewed against prescribing guidelines, but response was poor, and it was a challenge to understand the risk factors in order to suggest ways to reduce community CDI. Therefore, a pilot was trialled in March and April 2024 to gather this information from GP’s on each case using a less time consuming process, that would collate data and provide presentation graphs to support the findings. Changes and updates were made on the feedback, and the Community onset C.difficile analysis 2024/25 was launched on 1st April 2024.
Questions included in the Community onset CDI analysis 2024/25 MS Form
- What was the date the sample was taken?
- What date was the result available to the practice?
- Please select all risk factors for CDI applicable to this patient. (drop down list)
- Was the patient a resident of a Care or Nursing Home?
- Is there any relevant underlying morbidity as listed? (drop down list)
- How many days prior to the sample did the patient become symptomatic?
- Was there a delay in sampling?
- Has the patient had a previous episode of CDI or C diff colonisation (GDH positive on lab result)?
- Has the patient consulted their GP in the 3 months prior to the positive result?
- If so, what was this due to a respiratory infection? (if yes, then continued to…if No then to 15,18 and 19)
- Does the patient have a history of previous respiratory infections?
- Was a microbiology sample taken?
- Was the patient prescribed antibiotics in primary care for a respiratory infection? If so which?
- Was the antibiotic choice in line with SCAN guidance?
- Has the patient seen the GP within the last 3 months due to a Urinary tract infection? (if yes than same questions for respiratory as above and also…if no skip to 18)
- Did the patient have a urinary catheter of any kind, in the 3 months prior to CDI result?
- Was a urine dipstick performed to aid diagnosis of a UTI?
- Has the patient seen the GP within the last 3 months due to cellulitis or a skin / soft tissue infection?
- Has the patient seen the GP within the last 3 months due to a wound infection (including leg ulcers, diabetic foot ulcers and bites)? If so what?
- Has the patient seen the GP within the last 3 months due to a long-term condition?
- Has the patient had an inpatient episode in the last 3 months, if yes please forward Discharge Summary?
- Has the patient received chemotherapy in the last 6 months?
- What date was the treatment for CDI commenced?
- What treatment was prescribed and was this prescribed as per SCAN guidelines or following microbiologist advice?
- Was the patient taking a Protein Pump Inhibitors (PPI) within 3 months prior of the CDI result?
- Was the patient taking laxatives at the time of the sample?
- Was the patient taking Imodium or equivalent prior to the CDI result?
How to set up and MS Forms
Set up and MS Forms link. Suggested questions attached.
ICB – Setting up a dataset for your area (can be by non-clinical administration).
- After 16th of each month, download the UKHSA DCS report for the previous months CDI. (The deadline for trusts to upload data is 15th of each month, so to avoid missing cases, wait till 16th)
- Filter in the ‘Community Onset – Community Associated’ (COCA) and the ‘Community Onset – Indeterminate Association’ (COIA) in column BO ‘Apportionment Rule Category’ only.
- Select
- Save onto an excel spreadsheet and password protect as will contain PID.
- Title the columns Unique ID, Specimen date, GP Practice, Pt name, DOB, NHS No, Request date sent, Request date received, Reminder request sent. You may want to separate areas or by acute trusts, e.g. BU0001 or OX0001 for 2 different counties.
- Fill in the name of the GP practice for each case.
- Send an email using the template below with the appropriate Unique ID number and patient details to each GP. Use Subject heading ‘‘Name of GP surgery’ request for information’.
- Add date request sent to excel spreadsheet and a column to add when the GP responded. Reminders can be sent to non-responders the following month.
Providing reports
Log on to MS Forms
Click on responses (top left corner), download a copy in excel Remember to date/ID spreadsheet, as responses will continue to be submitted), select appropriate graphs required and add context from the responses. Check and share your form results.
Email template used to send to GP’s
Dear Name of GP practice
Please forward to the patients’ GP.
Dear Doctor
Your patient (xx), NHS No 000-000-0000, DOB xx/xx/xxxx, tested positive for C.difficile infection (CDI) on xx/xx/xxxx. Please copy the ID AB0000 and paste into this link to complete the investigation into this community onset categorised CDI sample. We appreciate that this patient may not have had contact with primary care recently, but we would appreciate your feedback in order to understand risk factors and reduce CDI categorised as community onset. Further information regarding CDI can be found here.
Please take this opportunity to review the indication for any long-standing prescription. The risk of CDI relapse is high, so please consider any antibiotic prescription very carefully and avoid where possible. There is evidence that PPIs may be a risk factor for CDIs, although this is not conclusive. CDI treatment guidelines are available through Eolas.
This data gathering process is designed to be less time consuming for GP’s, it supports the delivery of Regulation 12: Safe Care and treatment (CQC) and Criteria 1 of the Code of Practice. Any learning from analysis of CDI cases should be included in the practices Annual Infection and Prevention Control Statement. An anonymised report of the finding from this Community CDI Analysis is published quarterly in the GP Bulletin and presented at the ICB quarterly Infection Prevention Control Committee.
To enhance our Antimicrobial Stewardship efforts, BOB ICB, in collaboration with BOB ICS, have developed a patient information leaflet. This leaflet can be sent directly to patients’ mobile devices at the time of prescribing antibiotics, or alternatively there is a printable version of the same. Please ensure you save this link in a convenient location for easy forwarding to patients as needed.
When recording CDI, please use Snomed code: Clostridioides difficile infection 186431008
On completion of the form, please submit and click on the 3 dots in the top right-hand corner, click on print and from the drop down, save as a PDF for your records.
Please email bobicb.ipc@nhs.net if you have queries about this form or would like to provide feedback. We would value your comments on how the form can be improved.
Kind regards
Suggestions
- Set up a spreadsheet with all GP generic email addresses for ease of process
- As described above, maintain a protected spreadsheet of all UKHSA DCS, COCA and COIA with Unique ID, date of CDI, patient, name, NHS No, DOB, GP, when request sent, whether request received, date reminded if needed.
- Every month check which GP’s have not responded to the request and send a gentle reminder, add date reminder sent to the main spreadsheet, ideally one reminder and then cease.
Further any further information please contact Hilary Munube bobicb.ipc@nhs.net
References
- Annual epidemiological commentary: Gram-negative, MRSA, MSSA bacteraemia and C. difficile infections, up to and including financial year 2023 to 2024.
- Clostridioides difficile infection: antimicrobial prescribing NICE
- Clostridium difficile infection: risk with broad-spectrum antibiotics NICE
- The use of faecal microbiota transplant as treatment for recurrent or refractory Clostridium difficile infection and other potential indications. Joint British Society of Gastroenterology (BSG) and Healthcare Infection Society (HIS) guidelines
- UK 5-year action plan for antimicrobial resistance 2024 to 2029, UK
Further Reading
- Recent work has demonstrated that numerous cases are missed, either due to inadequate diagnostic tests or lack of clinical suspicion.
- A point-prevalence study on community and inpatient Clostridioides difficile infections (CDI) – support recommendations for improving diagnosis in patients presenting with diarrhoea in the community, to guide good practice to limit the spread of CDI.
- European study – Improving care for patients with Clostridioides difficile infection – A clinical practice and healthcare systems perspective concluded:
- Limited integration between primary and secondary care can delay diagnosis and treatment
- Awareness about CDI diagnosis and treatment can be low, especially among primary-care providers
- Recurrent Clostridium difficile Infection: Risk Factors, Treatment, and Prevention, Jung Hoon Song, You Sun Kim https://pmc.ncbi.nlm.nih.gov/articles/PMC6346998/#:~:text=2.-,Use%20of%20antibiotics,difficile%20after%20CDI%20diagnosis.&text=A%20meta%2Danalysis%20showed%20that,2.05%3B%20p%3C0.00001).
